Payer denials are not new to revenue cycle leaders. But DRG downgrades represent a particular kind of threat: one that often arrives quietly, weeks after discharge, buried in a post-payment adjustment. By the time your team catches the downgrade, the revenue has already walked out the door.
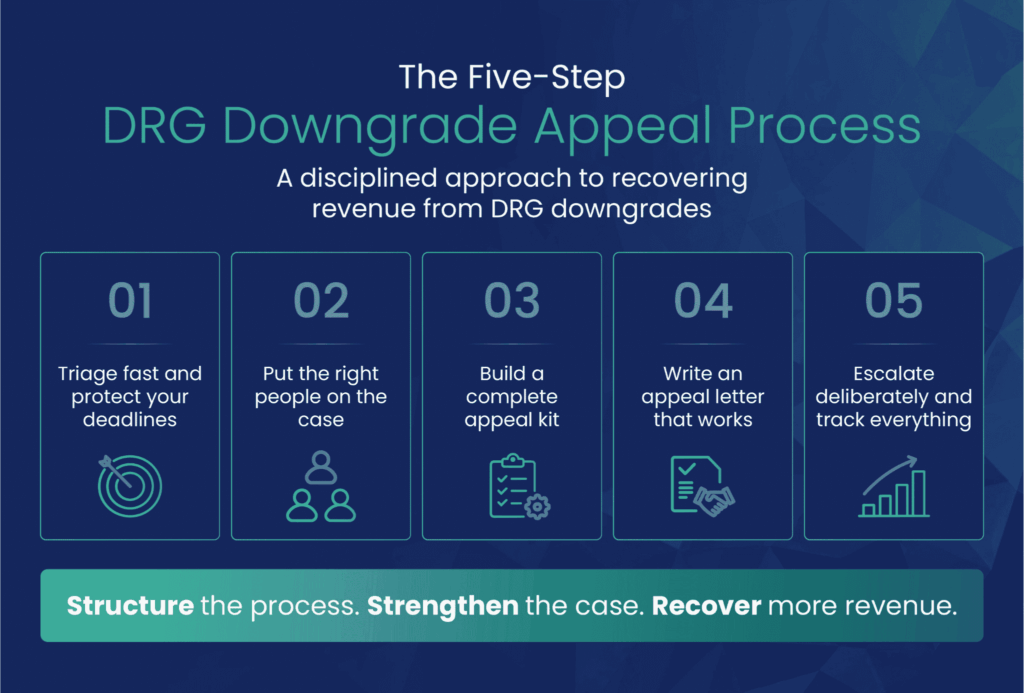
This guide walks through the DRG downgrade appeal process from triage to escalation, with a focus on what truly moves the needle for revenue cycle teams. You will learn how to identify the highest-risk DRGs, build a defensible appeal, and put the right people on the right denial type. More importantly, you will learn how to stop treating appeals as one-off firefighting and start running them as a systematic revenue recovery function.
According to the American Hospital Association, Medicare Advantage claim denials increased 55.7% between 2022 and 2023, while commercial denials rose 20.2% over the same period.
Hospitals spent nearly $18 billion in 2025 alone fighting to recover payments they had already earned. For a revenue cycle operation running on thin margins, that is not sustainable.
The good news is that this is a winnable fight. A 2024 Premier Inc. analysis found that more than 54% of denied claims are ultimately overturned. The hospitals recovering revenue share one thing in common: A systematic approach to appeals.
An outright denial is visible. A DRG downgrade is not. Payers conduct retrospective reviews and reassign a lower-weighted DRG, often weeks or months after the claim was paid. The result is a quiet, compounding revenue drain that can be easy to miss in a high-volume environment.
The downstream consequences extend beyond individual claims. Repeated downgrades suppress your Case Mix Index (CMI), signaling to payers and regulators that your hospital serves a less complex patient population. A lower CMI reduces prospective payment rates, weakens your negotiating position with commercial payers, and can invite additional scrutiny. One downgrade is a billing dispute; a pattern of downgrades is a strategic liability.
Medicare Advantage plans have been the most aggressive in pursuing these adjustments. What many hospitals do not fully leverage is that CMS rules require MA plans to follow standard Medicare coding policies and ICD-10 guidelines. That is not just regulatory background; it is a direct line of defense in your appeal. The threat has grown more sophisticated in recent years.
Payers are increasingly deploying automated algorithms and AI-driven audit tools to flag and downgrade DRGs at scale, often before any human clinical reviewer touches the claim.
The AHA has specifically identified machine learning algorithms as a driver of denial growth, noting that poor applications of these tools result in automatic denials without consideration of a patient's individual clinical circumstances or review from a clinician or plan medical director.
For revenue cycle teams, this changes the nature of the appeal. When a denial originates from an algorithm rather than a physician reviewer, the response strategy is different. You are not rebutting a clinical judgment; you are challenging an automated decision that may have applied rigid criteria without accounting for the full complexity of the case. That distinction matters when building your appeal, selecting your escalation path, and deciding when to request a peer-to-peer review.
Payers do not audit randomly, but rather they concentrate reviews on high-weight DRGs where a downgrade yields the largest financial return. Understanding which cases carry the most exposure is the first step toward protecting rightful revenue reimbursement.
The diagnoses that consistently draw the most scrutiny include sepsis, acute respiratory failure, acute kidney injury, severe malnutrition, and type 2 myocardial infarction.
Type 2 MI is frequently targeted because demand ischemia is often documented as a secondary finding rather than the principal diagnosis, and payers require specific documentation linking the underlying cause to the MI designation. Severe malnutrition denials turn on whether the record explicitly supports the criteria for that severity level, including the specific indicators the clinician used to arrive at that diagnosis, such as weight loss, reduced intake, or functional decline.
In both cases, a concurrent CDI query during the encounter is far more effective than a post-discharge appeal. Trauma cases and patients requiring ECMO are also high-risk, given the complexity of documentation those cases demand. These are not obscure edge cases; they are common high-acuity admissions that appear in nearly every inpatient facility.
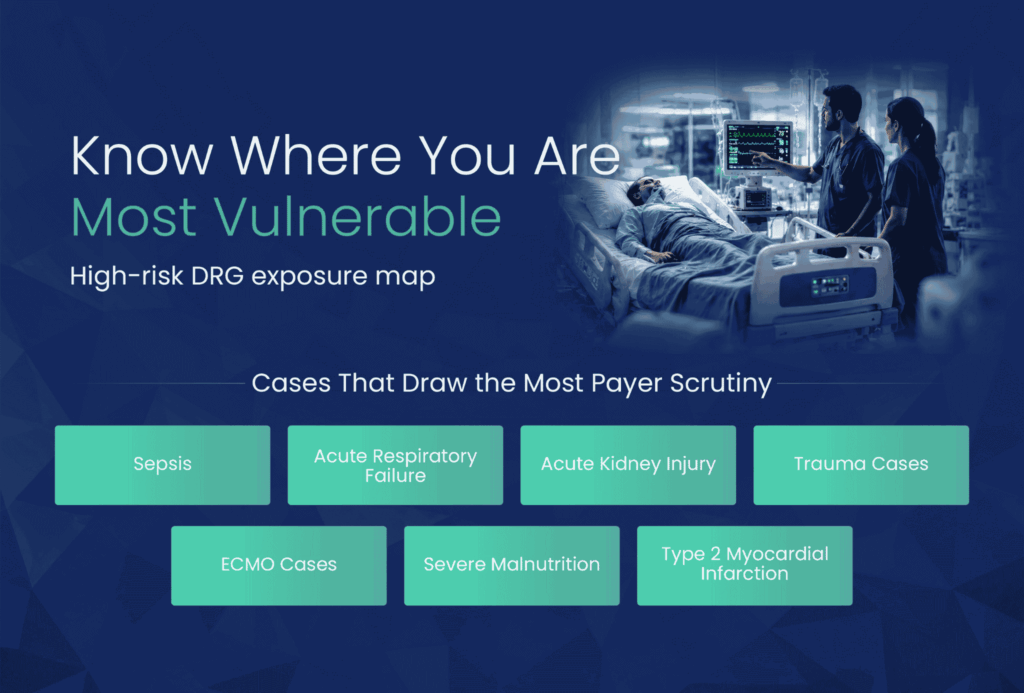
Overturning a sepsis downgrade can recover between $3,000 and $7,000 per claim. Multiply that across volume, and the revenue impact becomes clear.
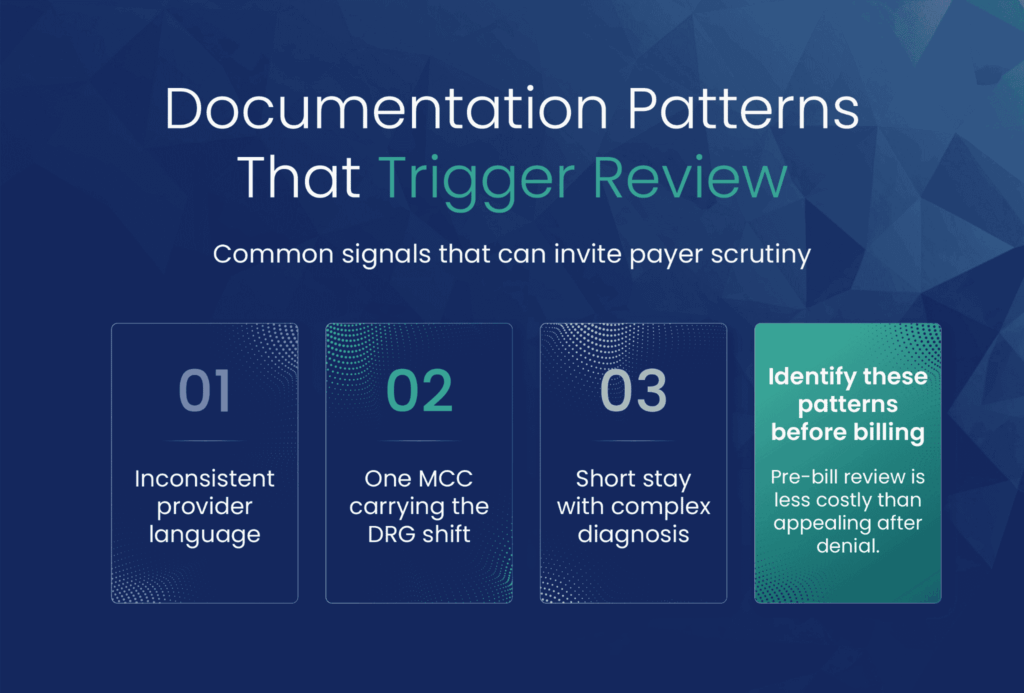
Certain documentation patterns invite denials even when the clinical picture is straightforward. Inconsistent language across providers, a single MCC carrying the entire DRG shift, and a short length of stay paired with a complex diagnosis are all triggers that flag cases for payer review. Identifying these patterns before billing is far less expensive than appealing them after.
Before building an appeal, your team needs to answer one question: What kind of downgrade is this?
There are two distinct types, and they require fundamentally different responses. Getting this wrong is one of the most common and costly mistakes in the appeals process.
The first is a coding-based downgrade. The payer disputes the ICD-10 code assignment itself: the sequencing of diagnoses, the selection of a CC or MCC, or the application of coding guidelines. These appeals are built on ICD-10-CM Official Guidelines, AHA Coding Clinic references, and UHDDS definitions. A strong coder and CDI specialist can lead this defense.
The second is a clinical validation denial. Here, the payer is not challenging the coding; it is challenging whether the clinical evidence in the record supports the diagnosis at all. A common example is sepsis: A case documented under Sepsis-2 criteria may be denied by a payer applying the narrower Sepsis-3 standard.
ICD-10-CM Official Guidelines and AHA Coding Clinic do not require Sepsis-3 criteria for diagnosis coding, meaning a payer applying a Sepsis-3 threshold is imposing a standard that exceeds CMS coding guidance and is a contestable overreach, not a legitimate basis for denial.
This type of denial requires a physician advisor to lead the response, with a clinical narrative that addresses the acuity of the case in medical terms.
Some denials combine both elements. Recognizing that early allows you to mobilize the right resources without losing time.
The moment a downgrade is identified, the clock is running. Appeal windows vary widely by payer, from 30 days to one year, and a missed deadline forfeits your right to dispute entirely. Deadline management is not an administrative detail; it is a revenue protection function.
For Medicare fee-for-service, the process follows a five-level path:
Medicare Advantage plans are required to provide the same five-level structure under CMS rules. For commercial payers, appeal rights are contract-specific, so reviewing the payer agreement and the explanation of benefits language is an essential first step.
Your triage process should identify the downgrade type, assign the right team, and confirm the deadline before anything else moves forward.
The appeal team should match the denial type. For a coding-based downgrade, that means your lead coder and CDI specialist. For a clinical validation denial, a physician advisor is not optional; it is the foundation of the appeal. Payer medical directors respond to peer-level clinical arguments in ways they simply do not respond to coding citations alone.
Before launching a formal written appeal, consider requesting a peer-to-peer review with the payer's medical director. This step alone resolves a meaningful share of clinical validation disputes and avoids the time and cost of a full written escalation. A revenue cycle lead should own the process end-to-end: tracking deadlines, coordinating team members, and managing escalation timing.
One of the most consistent findings in DRG downgrade cases is that payers issue denials without having thoroughly reviewed the medical record. Do not assume they have read it. Submit the complete record with your appeal and make the relevant clinical evidence impossible to overlook.
Start with a clinical timeline: from the patient's ED presentation through labs, imaging, treatment decisions, and clinical course. Then layer in the objective markers specific to the diagnosis in question.
Pair the clinical evidence with authoritative coding references: The ICD-10-CM Official Guidelines from CMS and relevant AHA Coding Clinic guidance. Then pull the payer's own medical policy and identify precisely where the record meets their stated criteria. Finally, annotate the denial letter directly, addressing each stated rationale with a specific, documented rebuttal.
The appeal letter is where the case is won or lost. Structure matters as much as content.
Open with the regulatory grounding: the applicable ICD-10-CM coding guidelines, UHDDS principal diagnosis definitions, and, for MA plans, the CMS requirement to follow standard Medicare coding rules. Establishing the governing framework early tells the reviewer this appeal is built on policy, not preference.
Then tell the clinical story. Narrate the acuity of the case: what the patient presented with, how the clinical picture evolved, what treatment decisions were made and why. A list of diagnosis codes does not convey complexity. A well-constructed clinical narrative does.
Address the payer's denial rationale directly and specifically. Ignoring their argument signals weakness; dismantling it signals command of the case.
For clinical validation denials, lead with the physician advisor's attestation and let the clinical evidence carry the argument. Throughout, keep the tone professional and factual. Adversarial language rarely helps and can invite dismissal at the first level of review.
Most hospitals stop appealing after the first denial. That is exactly what payers count on. The data supports persistence: Over 54% of denied claims are eventually overturned, with commercial payers reversing more than 60% of initial denials. The revenue is there to be recovered.
Know your escalation path and the timing requirements at each level before you need them. ALJ hearings and external reviews are not last resorts; they are legitimate tools that frequently produce favorable outcomes for well-documented cases.
Treat every payer interaction as part of the record: Log dates, contacts, responses, and outcomes. Over time, this data becomes your pattern file, revealing which payers are systemically downgrading specific DRGs and building the case for a broader response.
Note: Under CMS-4208-F, which was made effective January 1, 2026, once an MA plan approves an inpatient admission, it generally cannot reverse that approval based on information gathered after the fact. Plans may normally reopen only for fraud or obvious error. Hospitals that are not aware of this protection may be conceding mid-stay reversals they no longer have to accept.
Winning appeals is important; not needing to appeal is even better.
The most effective strategy is pre-bill clinical validation review for every high-risk DRG before the claim goes out. CDI involvement should be concurrent, not retrospective; documentation gaps are far easier to close during the encounter than after discharge.
Engaging physicians directly, and showing them specifically how their documentation affects reimbursement and audit exposure, is one of the most effective CDI tactics available.
CMS updates DRG logic, CC/MCC designations, and documentation requirements every fiscal year through the IPPS final rule. Annual training for coding and CDI staff on those updates is not optional if you want to avoid preventable denials.
The PEPPER report, a free CMS benchmarking tool, allows hospitals to compare DRG coding patterns against national norms; coding within normal ranges is both a compliance indicator and a defense against payer scrutiny.
Track denial trends monthly by payer, DRG, and diagnosis. A pattern of downgrades on a specific DRG from a specific payer is not a coincidence; it is a signal of systemic audit activity, and for public payers, it can precede recoupment extrapolation across a broader population of claims. Getting ahead of that pattern is less expensive than responding to it.
Building appeal kit templates for your highest-risk DRGs removes the friction from the process. When a denial arrives, your team should not be starting from scratch; they should be activating a documented workflow.
DRG downgrades are not inevitable losses. They are recoverable revenue, and the hospitals capturing that revenue are the ones that treat appeals as a systematic revenue protection function rather than a case-by-case administrative burden.
Every uncontested downgrade is a permanent write-off. Every pattern left untracked is a compliance risk. And every dollar recovered through a successful appeal is proof that the investment in a disciplined DRG audit process returns far more than it costs.

About the author
Kelsey Taylor, BSN, RN, is the Senior Director of Clinical Denials at EnableComp, bringing over 10 years of experience in healthcare management and clinical operations to the role. Her background spans clinical quality, care management, and product management, giving her a well-rounded lens on how revenue cycle, training, and clinical operations intersect. She's passionate about empowering teams to deliver patient-centered, impactful results and frequently speaks on topics like DRG revenue integrity, complex revenue recovery, and denial prevention strategy.