You don't need to be convinced that denials are a problem. You're living it.
In a recent survey of hospital and health system executives, nearly 81% reported that rising denial rates are a major stressor. The frustration is real, and so is the revenue walking out the door.
What makes the problem more difficult is that most providers don't have a clear view of what denials are actually costing them. Blended metrics that lump routine administrative denials together with complex clinical disputes can make overall performance look stronger than it is, while significant revenue leakage goes undetected.
Then there's the cost of fighting back. Appealing a denial isn't free, and for high-volume environments, the math on whether to pursue a claim isn't always straightforward. Meanwhile, payers are getting faster and more sophisticated, and most hospitals are not keeping pace.
This article cuts through the noise with the denial statistics every CFO should have on their radar: where revenue is slipping through the cracks, why the full scope of the problem is so difficult to see, and what leading health systems are doing differently to get ahead of it.
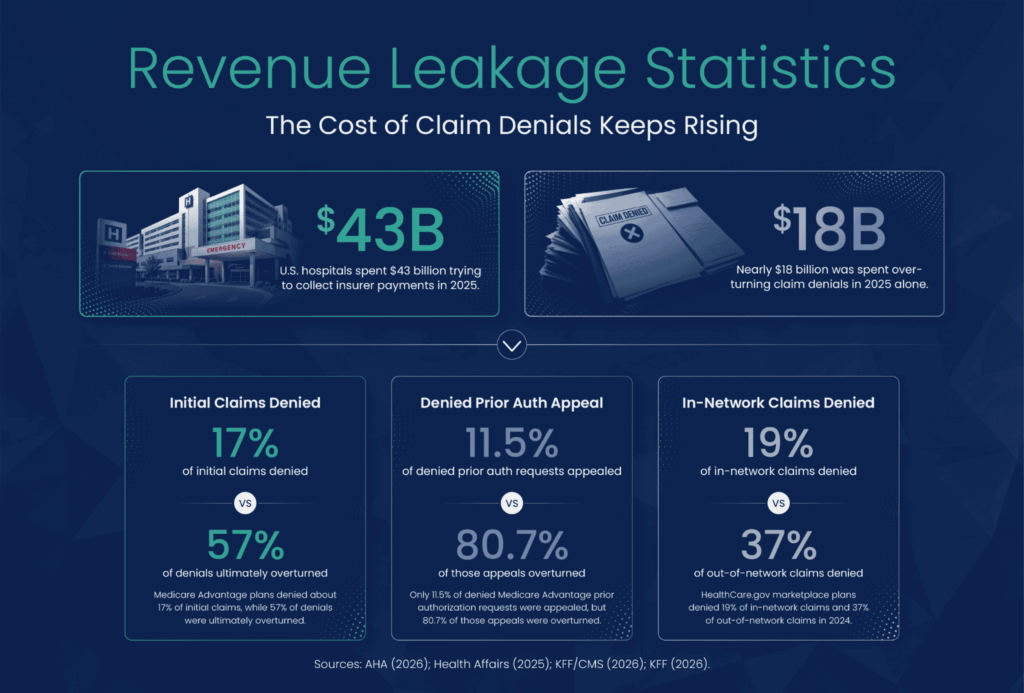
Denial pressure is broad-based, with strong independent signals from Medicare Advantage and the ACA marketplace. A Health Affairs analysis found that Medicare Advantage plans denied approximately 17% of initial claims, with 57% ultimately overturned.
KFF's analysis of CMS transparency data found that HealthCare.gov marketplace plans denied 19% of in-network claims and 37% of out-of-network claims in 2024. The same report found that administrative reasons accounted for 25% of in-network denial reasons, reinforcing the need to separate preventable denials from more complex payer disputes.
For hospital finance leaders, rising denial rates are not only an operational problem; the dollars behind those denials are a cash problem. When those dollars remain unresolved or fall out of appeal workflows, the result is revenue leakage.
High-level denial reporting has value, but it can mask leakage.
While the cost of processing a routine claim is typically around $7 to $10 across payers and providers, EnableComp, which specializes in RCM complexity, estimates costs for processing a complex claim can be three to ten times that, with some claims costing even more. That spread matters because complex denials often require clinical review, coding expertise, regulatory knowledge, and payer-specific escalation.
When standard and complex denials are grouped, high-volume administrative recoveries can make performance look strong, while a smaller set of complex cases creates disproportionate exposure.
In 2025, U.S. hospitals spent $43 billion trying to collect payments from insurers for care already delivered.
The average cost to rework a denied claim is between $25 and $181. Overturning claims denials costs hospitals nearly $18 billion in 2025 alone.
For high-volume denial environments, those rework costs compound quickly, leaving revenue cycle teams to weigh whether each claim is worth pursuing. It's a calculation that doesn't always get made accurately or at the right scale.
Only 11.5% of denied Medicare Advantage prior authorization requests were appealed, and of those, 80.7% were overturned. The appeal process works, but resource constraints and ROI concerns quietly push recoverable revenue off the table before the fight even starts.
For hospitals operating under margin pressure, unworked denials become write-offs. Complex cases routed into standard queues can age past the point of recovery, and reimbursement for delivered care provided never arrives.
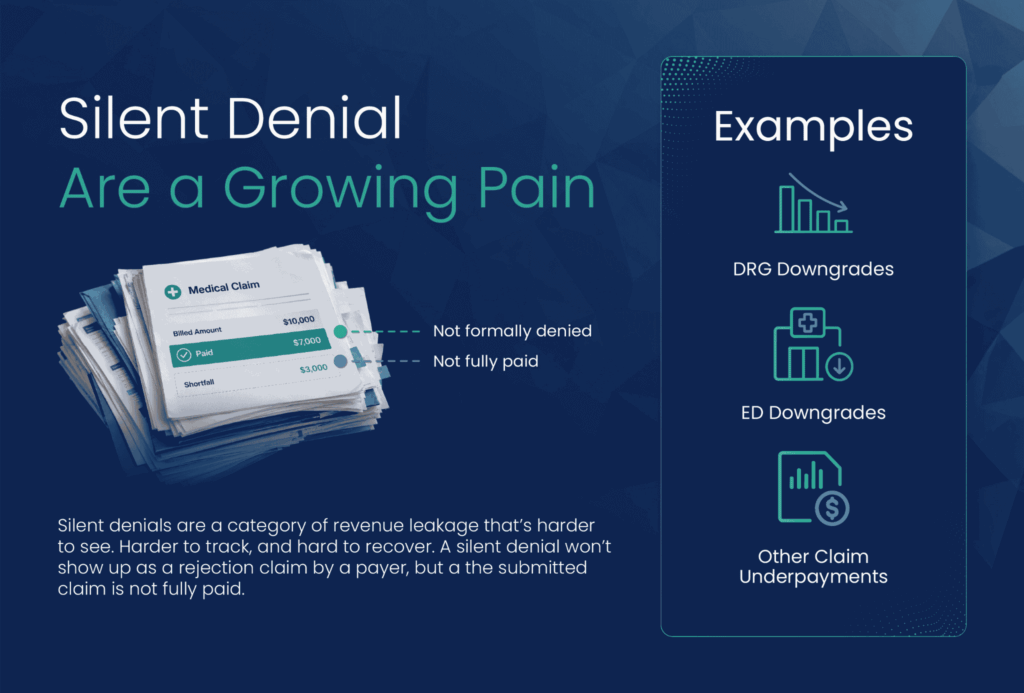
Not every revenue loss shows up as a denial. A silent denial won’t show up as a rejected claim by a payer, but the submitted claim is not fully paid either.
DRG downgrades, Emergency Department (ED) level-of-care downgrades, and other underpayments arrive as payment reductions rather than formal denial notices, which means they often bypass the workflows built to catch them. For many hospitals, these losses are hidden in plain sight.
DRG downgrades alone can represent significant dollars per claim. When a payer recodes a case to a lower-weighted diagnosis, the revenue difference rarely triggers the same urgency as an outright denial, even when the financial impact is comparable or greater. The same is true for ED downgrades, where payers reduce the level of care billed without issuing a formal denial that revenue cycle teams would typically flag and pursue.
Silent denials are a category of revenue leakage that's harder to see, harder to track, and harder to recover. Many hospitals aren't measuring it at all, not because they're not paying attention, but because their denial management systems weren't built to surface it. If your team is only tracking what's formally denied, you're likely underestimating your total exposure by a meaningful margin.
Payers are using AI and advanced analytics to review claims across broader datasets and at faster speeds. A Stanford-led review evaluated 21 AI tools active across utilization review and described the dynamic as an "arms race." An NAIC survey of 93 large health insurers found that 84% were already using AI in their operations.
The question for providers is not whether to match payer AI with provider AI. Most organizations will not win an arms race based on technology alone. The more practical challenge is to understand how payer behavior is changing and direct expertise toward the claims that carry the greatest financial risk.
The pressure is not always where hospitals expect. Hospitals can strengthen the mid-cycle with better documentation, analytics, and earlier intervention. But technology alone will not close the gap.
Complex denials involving payer-specific audit patterns, post-payment adjustments, and clinical validation still require experienced review and clear escalation paths. For many organizations, working with RCM experts focused on complex denial categories is becoming a practical revenue-protection strategy.
The next generation of denial management is less about adding another appeal queue and more about building revenue intelligence around claims already in motion.
Leading organizations are treating denial management as more than a back-end collections process. The goal is not only to overturn more denials faster but also to understand which revenue is most at risk, where denial patterns are emerging, and where earlier intervention can prevent future write-offs.
That shift matters because treating every denial with the same level of effort is not a strategy. The advantage comes from better prioritization, earlier intervention, and the ability to learn from denial patterns over time.
When denial rates climb, the answer is not simply to work faster. The stronger strategy is to segment denials by complexity, recoverability, and financial risk. Here’s where to start:
Registration, data verification, and prior authorization errors remain common causes of claim denials. Real-time eligibility checks, cleaner intake workflows, stronger authorization tracking, and better documentation practices can prevent many routine denials before they reach the payer.
Separating standard denials from complex clinical and payer-specific denials lets revenue cycle teams track each category by dollar value, recovery rate, time to resolution, and aging. Specialized resources should be directed toward the claims with the highest financial risk and strongest likelihood of recovery.
Denial management depends on coordination among patient access, clinical documentation, coding, case management, finance, and payer teams. Complex denials often require clinical judgment, coding expertise, and payer-specific knowledge, making cross-functional accountability essential.
Technology should help teams see patterns earlier, not just move denied claims through a queue faster. Hospitals need to understand which payers are changing behavior, which categories are growing, which service lines are most exposed, and which claims are most likely to recover before write-offs accumulate.
The goal is to move from chase-and-collect to predict-and-prevent.
Denial rates are rising. Rework costs are increasing. Recovery is taking longer. Payers are also becoming more sophisticated in how they review, downgrade, and challenge claims. The hardest dollars to recover are often tied to complex clinical and payer-specific denials that standard workflows were not designed to resolve.
That is the real cost of claim denials: delayed cash, avoidable rework, premature write-offs, and complex cases that never receive the right review.
The organizations that perform best will not necessarily be those with the lowest denial rates alone; they will be the ones with the visibility, expertise, and processes to respond before recoverable revenue is lost.
Most denial management approaches treat all denials the same, and that's exactly where revenue gets left behind. EnableComp specializes in the complex denials that are hardest to see, hardest to fight, and most likely to be abandoned before recovery. That means DRG downgrades, ED downgrades, underpayments, and high-value clinical disputes that require specialized expertise and payer intelligence that most internal teams simply don't have the bandwidth to build.
The hospitals seeing the strongest recovery results aren't working harder; they're working on the right claims with the right resources. If your organization is ready to understand where your true denial exposure lies and how much of it is actually recoverable, that's exactly the conversation EnableComp wants to have with you. Contact us now.
About the author
Kelsey Taylor, BSN, RN, is the Senior Director of Clinical Denials at EnableComp, bringing over 10 years of experience in healthcare management and clinical operations to the role. Her background spans clinical quality, care management, and product management, giving her a well-rounded lens on how revenue cycle, training, and clinical operations intersect. She's passionate about empowering teams to deliver patient-centered, impactful results and frequently speaks on topics like DRG revenue integrity, complex revenue recovery, and denial prevention strategy.