By Brian Kenah, Chief Technology Officer, EnableComp
Everyone in healthcare revenue cycle is talking about AI, but few offer specifics about what their AI actually does, how it was built, or how it is improving revenue. Those are the questions that matter.
The wrong AI strategy carries a steep penalty today. The One Big Beautiful Bill Act is projected to pull nearly a trillion dollars out of Medicaid over the next decade, enhanced ACA subsidies have expired, and HFMA is calling 2026 a revenue cliff. On the other side of the table, payers are using advanced AI to review and deny claims at a speed and scale that a human team cannot match.
When every dollar you’ve earned on the care you’ve already delivered becomes more valuable, and the payer side is getting better at not paying, "we have AI too" isn’t an answer you should accept.
The sharper question for hospitals and health systems is this: Does the AI working on my revenue cycle measure up to the complexity it must handle?
EnableComp's AI Transformation is our answer to addressing the complexities you face. It lays out measured production results and a straight account of how we built an operating model that handles complex claims, clinical denials, and revenue recovery at enterprise scale.
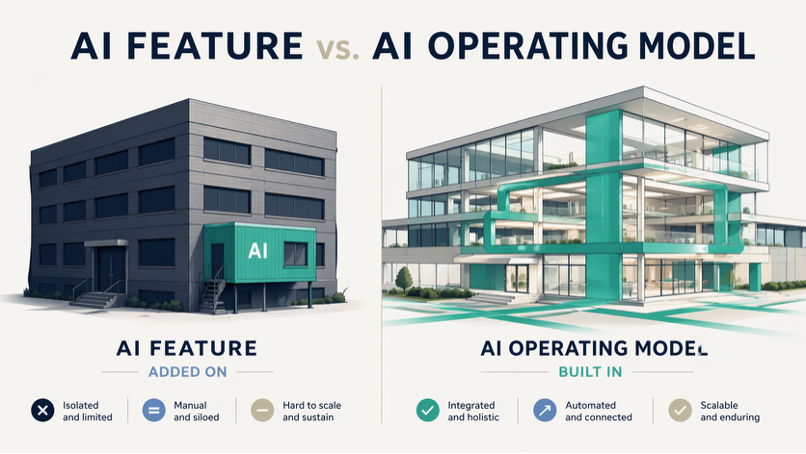
There is a significant difference between AI as a feature and AI as an operating model, and the distinction determines everything downstream.
A feature is a model here, an automation there. One step in one workflow gets faster, and the gain is linear: a little quicker, a little cheaper, a little less manual. Useful, but it doesn't change the economics
An operating model is different. Intelligence, automation, and domain expertise are integrated across the entire revenue lifecycle, and every cycle makes the next one smarter. The gains compound and performance accelerates over time rather than plateauing after the first release.
This distinction matters most when AI models get more capable, and nowadays they are getting more capable fast. Inside a feature, a better model makes one step a little sharper. Inside an operating model, a better model lifts the whole system, because the domain expertise underneath is suddenly being reasoned against by a stronger engine. The expertise doesn't change; the outcomes do.
Technology is commoditizing. Large language models, agent frameworks, and the tooling to stand up a development pipeline are all within reach, and a well-funded team can replicate any of it in months.
What doesn't commoditize is 25 years of operational knowledge about the parts of the revenue cycle that are hardest to work: complex claims, clinical denials, and revenue recovery on what was left on the table. Every state-specific rule, every payer-specific denial pattern, every appeal pathway, every workflow our most experienced specialists developed over decades, that is the codified expertise built into our system, and it cannot be quickly replicated.
We systematically converted that expertise into executable intelligence. The standard operating procedures didn't just inform the agents; they became them. Our agents don't follow scripts; they reason through complex situations. The judgment they apply comes from specialists who have worked on this for a quarter century.
The practical impact for hospitals and health systems is access to a system that already performs at a high level and keeps sharpening. Every process refined, every edge case documented, and every specialist workflow encoded adds to what it already knows.
The series covers the full arc of EnableComp's AI transformation, from how we build the technology to what it delivers for our clients.
We developed an enterprise methodology for orchestrating specialized AI agents across the full software development lifecycle, not developers using copilots, but AI-driven development at enterprise scale. Today, six specialized agents are actively delivering across four engineering teams in our HIPAA-regulated environment, and the measured results are concrete: product requirements that took weeks or months now take days or hours, and architecture documentation that consumed full sprints now takes a single working session. This is the foundation everything else runs on: the system that builds the system.
We turned the methodology inward and used it to build the AI systems themselves, following the same document-driven pipeline, except the "code" being produced is another AI agent. The result is an agentic framework for healthcare revenue cycle built on 25 years of specialist expertise encoded into production systems. Starting with the business process rather than technology was the single most important sequencing decision we made. Launch accuracy on new agents moved from roughly 50% to 70% as a direct result, while disciplined refinement has taken some agents to 95% on complex processes.
This is where the operating model meets the bottom line, through two layers that reinforce each other. Agentic workflow automation handles the operational complexity of claims: intake, classification, data extraction, letter generation, appeals, and routing. Predictive intelligence identifies which claims to prioritize, which are likely to be denied before submission, and where intervention will produce the highest return. That combination is the shift from "chase and collect" to "predict and prevent," and it is where the compounding advantage kicks in as the system matures.
Additional papers in the series will go deeper on the technical architecture behind the platform and on the measurable client outcomes this operating model delivers. We'll announce those as they're ready.
If you lead technology at a healthcare organization, The Blueprint is your entry point; the orchestration pattern, the governance model, and the measured velocity results are there to compare notes against.
If you run revenue cycle operations, Intelligence at Scale is yours. It is the clearest case we can make that the system working your hardest claims is built on real, specialist-validated expertise rather than a generic model pointed at a workflow.
If you sit in the Office of the CFO, From Reactive to Predictive is where the dollars are: yield, cycle time, collectability, and the mechanism that drives each of them in the right direction over time. This is where AI connects to the bottom line on the hardest claims in healthcare.
If you invest in or advise healthcare technology companies, read the full series. The capability moat is visible across the papers, and no single installment captures it alone.
Every claim in this series is measured against production results, and where something is directional, we say so. Human specialists are in the loop on every consequential decision, by design, not as a compliance afterthought, but as a structural feature of how the system operates. Client data is not used to train public models; we built the architecture to make sure of it.
The goal of publishing this is not to tell anyone their current RCM vendor is bad. It is to raise the bar on what hospitals should expect from the systems handling their most complex revenue cycle challenges. Complexity isn't slowing down, payer sophistication is accelerating, and the systems working these claims, along with the clinical denials and recovery work behind them, must get as strong as fast as the problems are getting harder. That is the bar we set for ourselves. It is the reason we built EnableComp's AI operating model the way we did, and it is the reason we are opening up the playbook.